


















Stroke can occur after a sudden disruption of blood supply to a part of the brain, sometimes causing a loss of ability to move particular parts of the body [Face, arm, leg], inability to see or speak and sudden change in balance. There are three types of stroke that require immediate recognition. (1) Ischemic stroke: A blood clot forms and blocks the artery in the brain. (2) Hemorrhagic Stroke: It occurs when a brain blood vessel ruptures. (3) Transient Ischemic Attack [TIA]: It is a warning that ischemic stroke is impending because of narrowing of blood vessel causing flow disruption.
Globally, Stroke affects 33 million individuals every year with two-thirds of all strokes occurring in the developing countries. Over the last few decades, the burden of stroke has been increasing worldwide, especially in developing countries. In a developing country like Pakistan, the prevalence and incidence of stroke is not exactly known largely because of lack of healthcare data collection and availability. Unfortunately, health epidemiology is not an established field in developing countries. Review of the reported case series from the medical literature pertaining to stroke incidence in Pakistan, it is apparent that Pakistan likely has the world’s highest rate of stroke per capita. In a small series of stroke patients from Islamabad, the crude age-and sex-adjusted stroke incidence was found to be 95 per 100,000 persons per year during the years 2000 to 2016, with the highest incidence of 584,000 of 650,000 noted among individuals aged 75 to 85. However, ground reality speaks completely otherwise where we see younger age groups of either gender experiencing stroke. Higher prevalence of diabetes and hypertension starting at younger ages amongst the population could be a potential reason for the age disparity and stroke onset in Pakistan.

Lack of access to a national standardized ambulance transport service across the country considerably adds to patient morbidity & mortality in patients with neurological time barred emergencies.In developing country like Pakistan, we see ‘It’s God’s Will’ mindset at most hospitals and patient only receives basic medical management [Blood pressure, diabetes etc.] and are left to luck. Lack of National standardized Emergency Transport System contributes to worsening in Morbidity and Mortality when it comes to treating time barred emergencies like Acute Stroke/ Neuro Trauma, Heart attacks etc.
Unlike Pakistan, all over the world, there is only one Emergency Room/Department concept as all specialties [Medicine, Surgery, Neurosurgery, Neurology, Cardiology etc.] are available under one roof to deal with any emergency in a timely fashion. Frequently, more than one organ is affected and having all specialists in the Emergency Department yields better patient outcomes. We frequently see patients going with strokes to Cardiology specific institutes only to be told later that the symptoms are stroke specific and not heart. But by then it’s too late to offer any acute stroke specific therapies. Similarly, brain related fatal complications frequently take place following acute cardiac problems / procedures and no neurologists or neurosurgeons are available within the cardiac center to provide immediate treatment.
The overall death rate from stroke in industrialized countries among people over age 65 years is about 10%-12%. Improved preventive medicine and utilization of aggressive acute stroke interventions and therapies have in recent decades, led to a steady decline in stroke incidence in most developed nations since 1970. In developed countries, stroke incidence, its associated morbidity & mortality is constantly declining because of robust stroke awareness and aggressive therapies administered within the acute period. Creating more stroke survivors has been the mantra in the developed world compared to ‘Its God Will’ approach in developing countries.
Stroke is also a leading cause of long-term disability. Three quarters of all strokes occur in people age 65 or older, and the risk of stroke doubles each decade after age 55.
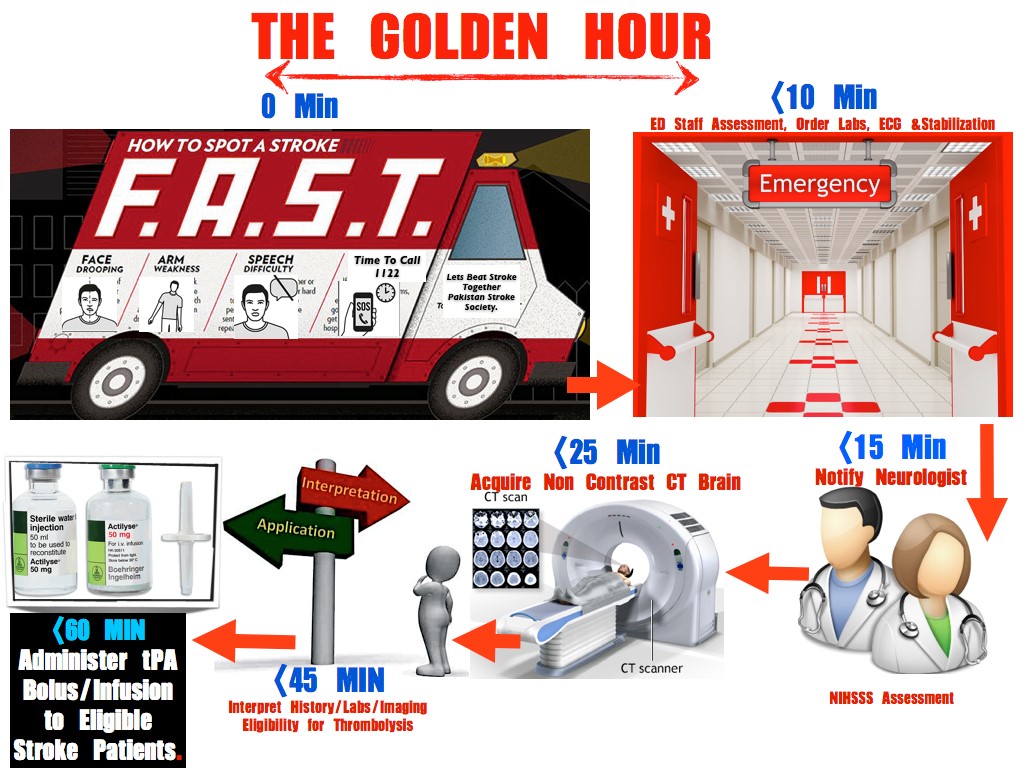
Acute Ischemic Stroke (AIS) treatment has been revolutionized in the last two decades with the increasing use of Intravenous Thrombolysis (IVT) and with the advent of Endovascular therapy (EVT). AIS treatment and outcome are time dependent and in the developed countries time saving measures are being implemented at every step of the treatment chain. These changes have resulted in lower treatment time’s in-hospital and excellent outcomes if stroke patients are treated within the Golden Hour i.e. treated within 60 minutes of symptom onset.
It is really good news that nearly 80 percent of strokes are preventable. Stroke is described as a “brain attack,” and is different from heart attacks. Brain Attacks [ischemic stroke] are predominantly painless while heart attacks present with severe chest pain. This difference should be recognized by both the patient and public at large so that the brain attack patient is transported to a dedicated Neurology department capable of treating acute strokes. Ischemic strokes are the most common variety, caused by a blockage of blood flow to the brain due to which brain cells near the blockage to die within minutes. If an acute evolving stroke is not treated within the first 6 hours of its onset, 2 [two] million neurons [brain cells] die every minute during stroke evolution. On an average ischemic stroke evolution can last up to 10 [ten] hours.
When it comes to Stroke
TIME IS BRAIN
Every 10 Minutes can SAVE
Up to 20 MILLION Brain Cells from permanent death.
| Brain Cells Lost | Number of Years the Brain Ages | |
| Per Stroke | 1.2 Billion | 36 Years |
| Per Hour | 120 Million | 3.6 Years |
| Per Minute | 1.9 Million | 3.1 Weeks |
| Per Second | 32,000 | 8.7 Hours. |
Both types of strokes [ischemic & hemorrhagic] are serious and require immediate medical care. A number of myths surround strokes, their causes and treatments. Many people think that strokes only affect older adults or that they are not treatable. The reality is that strokes can happen to anyone at any time, and proven treatments are available –But only if a stroke victim receives medical attention quickly and at the right medical facility.
The approach that you do not have to go to see a neurologist/doctor if stroke symptoms go away is the most dangerous myth associated with the Stroke. Temporary stroke symptoms are called transient ischemic attacks, or TIAs, and serve as an important warning sign prior to an actual stroke – a warning that needs to be taken seriously. Some call TIAs “mini strokes,” and they precede nearly 15 percent of actual strokes.
During a stroke, the part of the body controlled by the area of the brain experiencing the stroke stops functioning. Warning signs include sudden numbness or weakness of the face, arm or leg– especially on one side of the body.
Other symptoms include confusion, trouble speaking or understanding. The victim may have trouble seeing out of one or both eyes, and they may have difficulty walking or maintaining balance. A sudden, very severe headache might also be a sign of a stroke if there is no other cause.
If you think your loved one or friend might be having a stroke, Remember the Acronyms;
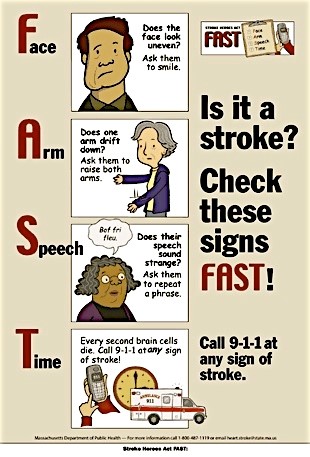
“B.E.F.A.S.T & F.A.S.T”
Balance: Ask the person if they are experiencing any balance issues or dizziness?
Eyes: Ask the person if they are having trouble with vision.
Face: Ask the person to smile. Does the side of the face drop?
Arms: Ask the person to raise both arms. Does one arm drift downward? Or is one arm difficult to raise up?
Speech: Ask the person to repeat a simple phrase. Is speech slurred?
Time: With any of these signs, call 1122 immediately. Using an ambulance with sirens saves valuable time.
Seek medical attention quickly if there is any suspicion of stroke. We, here at Services Hospital Lahore, have the motto “Stroke isn’t the End of Story – It’s just a Beginning”. Do not wait for symptoms to improve or worsen, instead note the time and call 1122 or area ambulance service immediately. A clot-busting medicine called IV [intravenous] tPA[tissue Plasminogen Activator] can be used for patients experiencing an ischemic stroke–but it must be given intravenously within 0-3 hours of stroke symptom onset.
The bottom line is that immediate medical attention is critical to improving the chances for stroke survival and lowering the chances for complications. Department of Neurology at the Services Hospital, Lahore has Acute Stroke Service line that provides 24×7 Stroke Care and does administer the clot busting tPA if patient arrives within the stipulated time frame [0-3 Hours] of symptom onset and meets the inclusion criteria. An Acute Stroke patient once identified has to undergo emergent CT Brain and some essential blood tests before being considered for clot busting medication administration. Hence, the earlier the stroke is identified, the earlier the treatment can start. Studies have shown, that earlier treatment shows significant improvement compared to those who come late to Emergency Department/hospital.
Some patients might also be eligible for a catheter-based procedures [Thrombectomy, Aspiration] to remove the blood clot, or other procedures to open up arteries narrowed by fatty deposits which reduces the chance of another stroke.
Nothing is better than Prevention. Preventing the first stroke or a recurrent stroke requires controlling modifiable lifestyle risk factors such as being overweight, smoking, physical inactivity, excessive alcohol use, intake of energy drinks and sodas and illicit drug use (cocaine, amphetamines, heroin etc.). Medical risk factors–many of which are directly related to lifestyle–include high blood pressure, high cholesterol, diabetes, sleep apnea and cardiovascular disease.
Controlling high blood pressure and diabetes are the most important things that can be done to prevent strokes. Thus, exercising, managing stress, maintaining a healthy weight, limiting sodium, sugar and alcohol intake, and taking prescribed medications are critical. Doctors might also prescribe preventative medications like antiplatelet drugs, anticoagulants, and cholesterol-lowering drugs, diabetes medications, CPAP machines for sleep apnea, and smoking cessation aids can also play a role.
For hemorrhagic strokes (brain bleeds), the risk factors are very similar, with high blood pressure being the leading cause. Head injuries, bleeding disorders and blood thinners are also additional causes. Catheters or surgery can be used to repair aneurysms or other vascular malformations associated with hemorrhagic strokes, and non-invasive stereotactic radiosurgery is also an option in certain cases.
After a stroke, recovery and rehabilitation efforts focus on restoring function to permit a return to independence. Physical, occupational, speech and cognitive therapy all play an important role in recovery and minimizing complications. Modifying risk factors to minimize the chance of another stroke is also very important. At the Department of Neurology, Services Hospital Lahore, patients are managed in dedicated Neurocritical Unit followed by both In-Patient & Out-Patient Rehabilitation. State of the Art Neurocritical & Neuro Rehab units have been established to help patients transition back to community with minimum to no dependence.
So while all strokes– large or small–should be taken seriously and acted on quickly, the good news is that they can be preventable and treatable.
Remember -Acute Ischemic Stroke Is a Treatable Condition.
“Stroke isn’t the End of Story – It’s just a Beginning”.



